All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub uses cookies on this website. They help us give you the best online experience. By continuing to use our website without changing your cookie settings, you agree to our use of cookies in accordance with our updated Cookie Policy
Introducing

Now you can personalise
your Multiple Myeloma Hub experience!
Bookmark content to read later
Select your specific areas of interest
View content recommended for you
Find out moreThe Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.







Integrating cilta-cel into earlier lines of therapy: Rationale and latest data from CARTITUDE-2 and CARTITUDE-4
Bookmark this article
Ciltacabtagene autoleucel (cilta-cel) is a B-cell maturation antigen (BCMA)-targeting chimeric antigen receptor (CAR) T-cell therapy, which is one of only two U.S. Food and Drug Administration (FDA)-approved CAR T-cell therapies for the treatment of relapsed/refractory multiple myeloma (RRMM). Both approved CAR T-cell agents are indicated in the heavily pre-treated setting after four or more prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.1
However, in February 2024, the European Medicines Agency (EMA) Committee for Medicinal Products for Human Use (CHMP) recommended the approval of cilta-cel after at least one prior line of therapy, including an immunomodulatory agent or proteasome inhibitor, for those who have progressed on the last therapy and are refractory to lenalidomide.1
The Multiple Myeloma Hub is pleased to summarize the rationale for and latest data from clinical trials of cilta-cel after one to three lines of therapy for the treatment of MM.
Rationale1
There are multiple justifications for the implementation of CAR T-cell therapies into earlier lines of therapy, including the potential to minimize mechanisms of resistance to CAR T-cell therapies (Figure 1).2
- Fitter T-cells
- Treatment with few prior lines of therapy is associated with improved persistence of CAR T-cells, and ultimately increased rates of myeloma cell death
- Increased immunogenicity of tumor cells
- Less pre-treatment heterogeneity in the antigen density expressed on tumor cells results in reduced resistant clone selection
- Lower tumor burden
- Implementation of CAR T-cells in earlier lines means tumor cells possess a lower proliferative potential
Figure 1. Mechanisms of resistance to CAR T-cells*
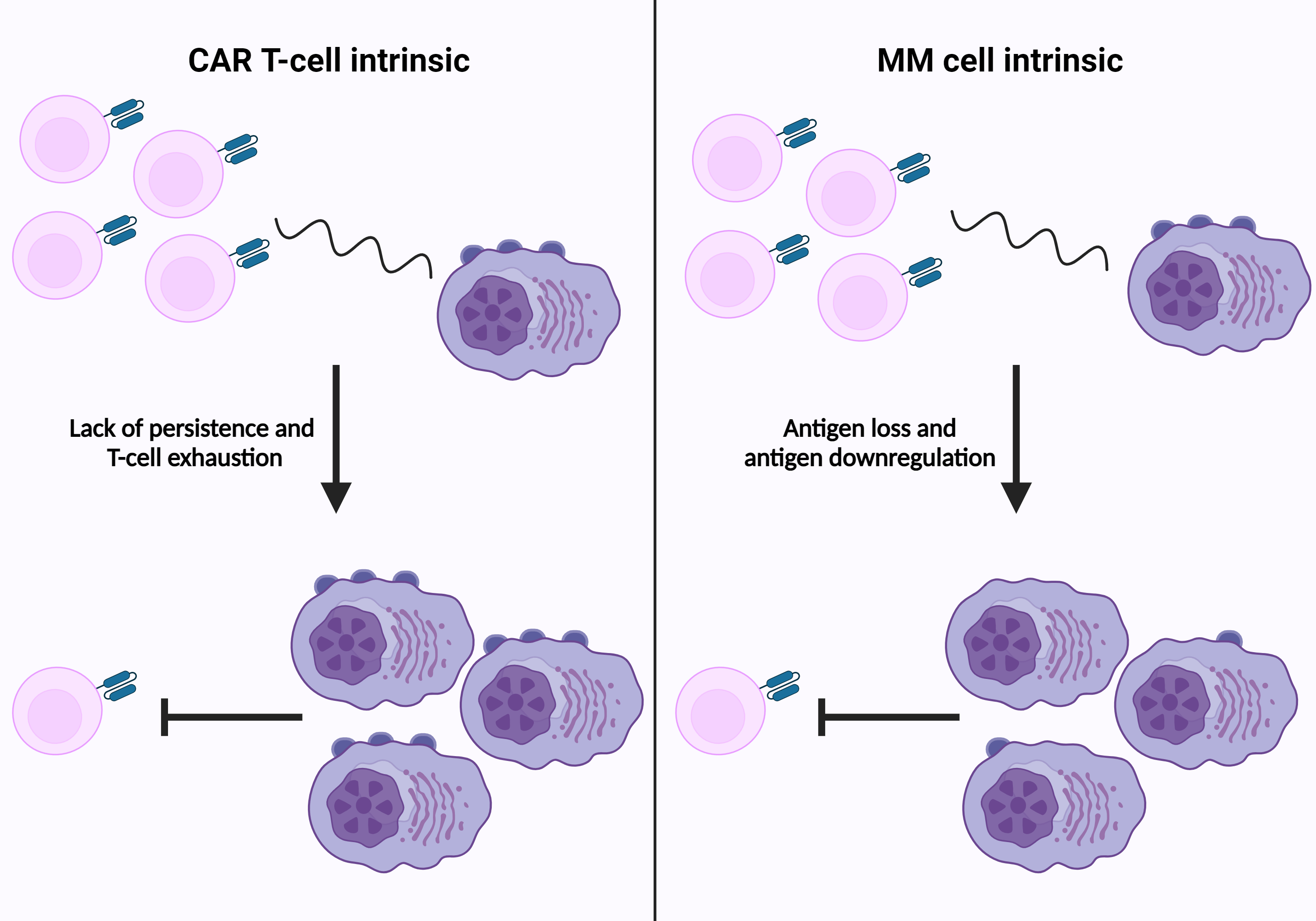
CAR, chimeric antigen receptor; MM, multiple myeloma.
*Adapted from D’Agostino and Raje.3 Created with BioRender.com.
Additional justifications for the implementation of CAR T-cells in earlier lines include the following:
- Better tolerability
- Less pre-treatment in MM has been shown to reduce the incidence of cytopenias, infection, and secondary malignancies
- Reduced tumor load is associated with reduced incidence of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), as well as a reduction in delayed neurotoxicity
- Impact of prior therapies on the efficacy of CAR T-cell therapies
- A difference in progression-free survival (PFS) rates of patients treated with CAR T-cell therapies is observed depending on pre-treatment (Figure 2)
- The PFS rates of patients treated with CAR T-cell therapies were particularly reduced when pre-treated with bispecific antibodies
- The later CAR T-cell therapies are delivered, the greater the likelihood of prior exposure to a therapy that negatively impacts PFS
Figure 2. PFS rates in patients treated with CAR T-cells by prior treatment*
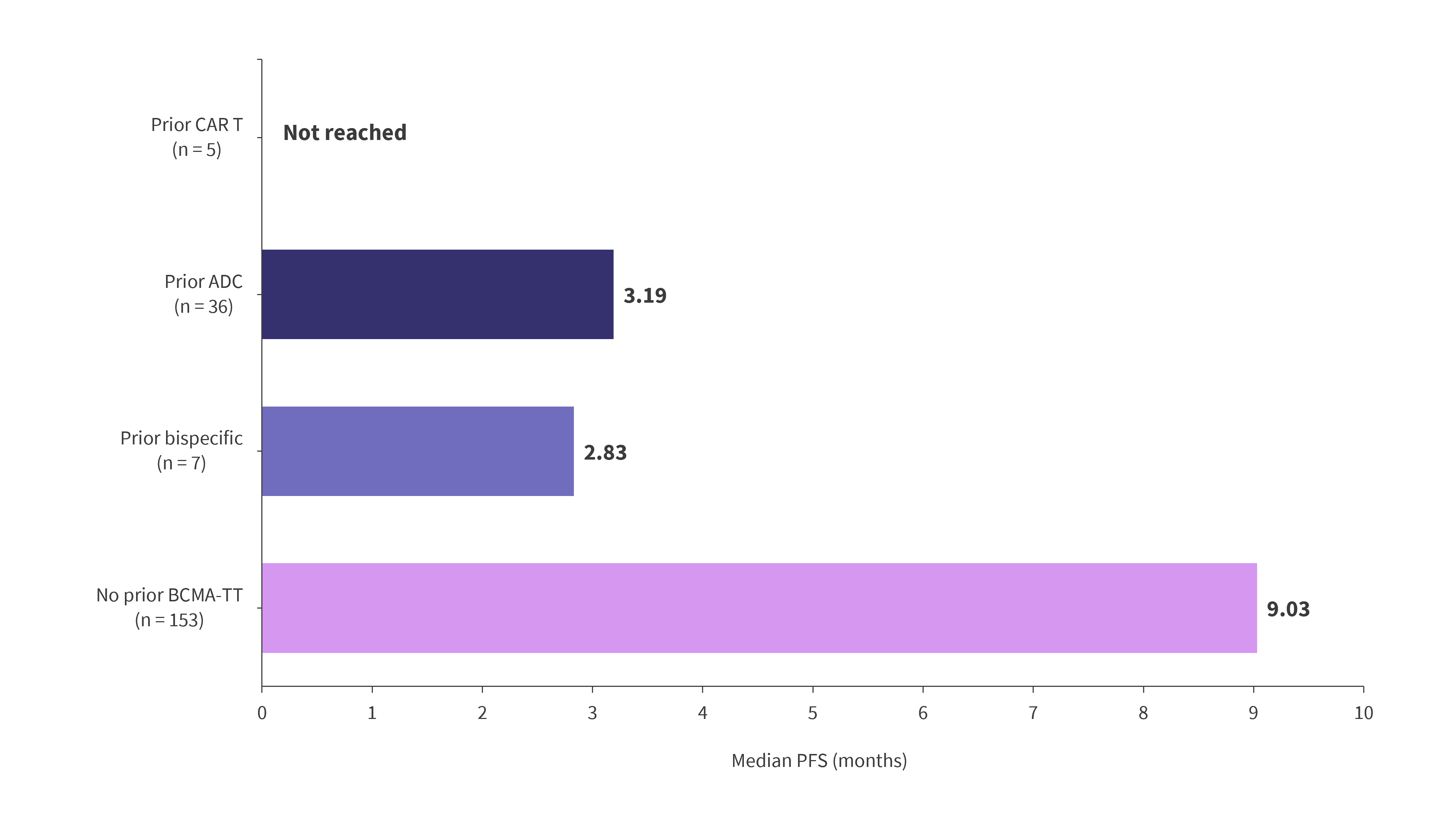
ADC, antibody–drug conjugate; BCMA-TT, B-cell maturation antigen targeted therapy; CAR, chimeric antigen receptor; PFS, progression-free survival.
*Adapted from Einsele.2
Additionally, there is an argument for implementing the treatments with the highest response rates in the earlier lines due to the lower documented attrition rates for therapy in the later lines (Figure 3). Notably, in Austria, 85% of patients with MM were unable to receive treatment beyond the third line of therapy, with similar data observed in the US, France, and Australia, highlighting the need for effective therapies in early lines where attrition rates remain high.2
Figure 3. Attrition rates for multiple myeloma therapies by line*
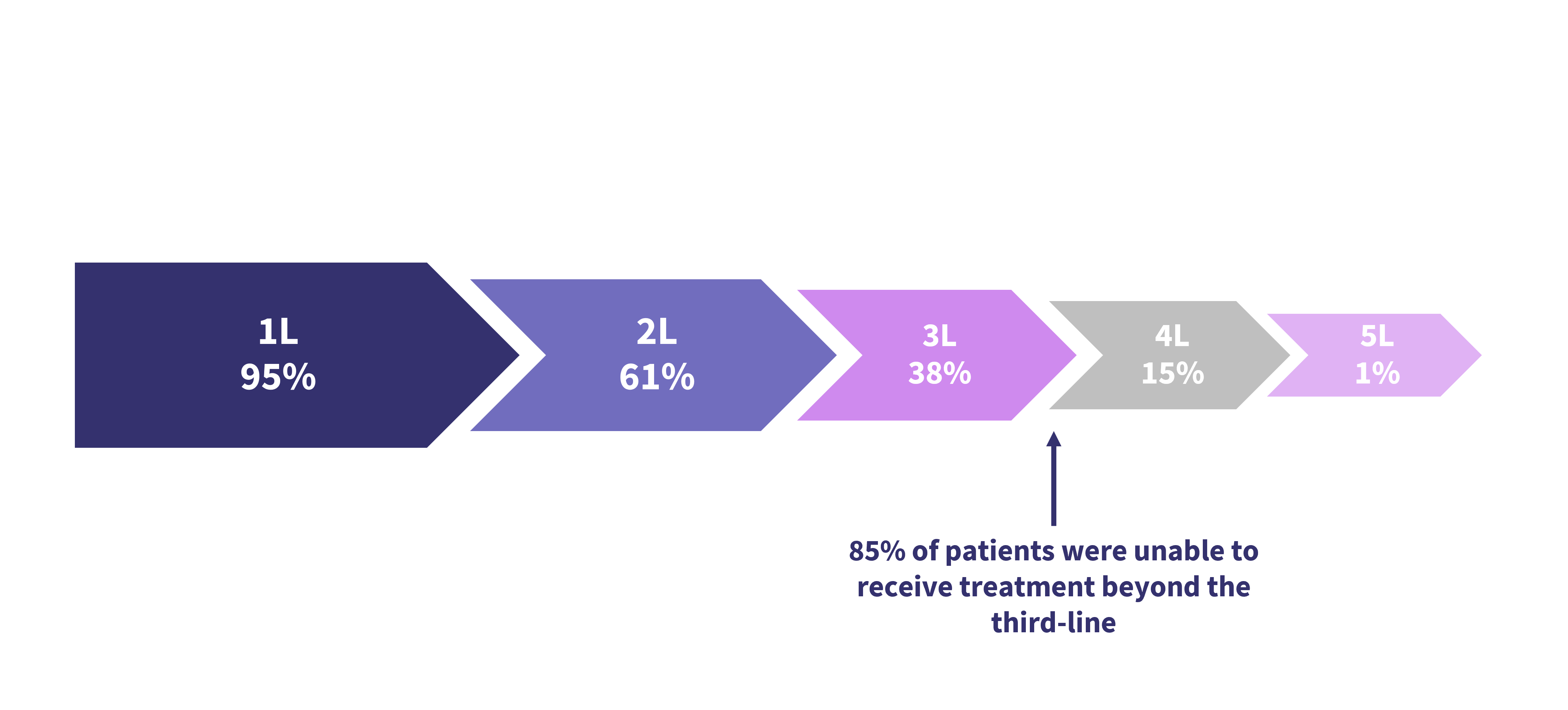
1L, first-line treatment; 2L, second-line treatment; 3L, third-line treatment; 4L, fourth-line treatment; 5L, fifth-line treatment.
*Adapted from Einsele.2
CARTITUDE-2
CARTITUDE-2 (NCT04133636) is a phase II, multicohort clinical trial evaluating the safety and efficacy of cilta-cel for the treatment of MM. Cohorts A and B included patients with one to three prior lines of therapy who are lenalidomide-refractory and those with early relapse at ≤12-months after autologous stem cell transplant or treatment initiation, respectively.
The trial design of CARTITUDE-2, including primary and secondary endpoints, has been reported previously by the Multiple Myeloma Hub here.
Efficacy4
At a median follow up of 29.9 months in cohort A and 27.0 months in cohort B:
- High rates of measurable residual disease negativity at a sensitivity rate of x10-5 were observed in both cohorts A and B at 100% and 93.3%, respectively.
- Sustained measurable residual disease negativity at ≥6 months was 40% and 52.6%, respectively.
- At ≥12 months, sustained measurable residual disease negativity was 35% and 36.8%, respectively.
- Response data was also consistently high, with slightly increased overall response rates observed in cohort B; however, a higher proportion of responders in cohort A experienced a stringent complete response (Figure 4).
Figure 4. Response rates in Cohorts A and B from CARTITUDE-2*
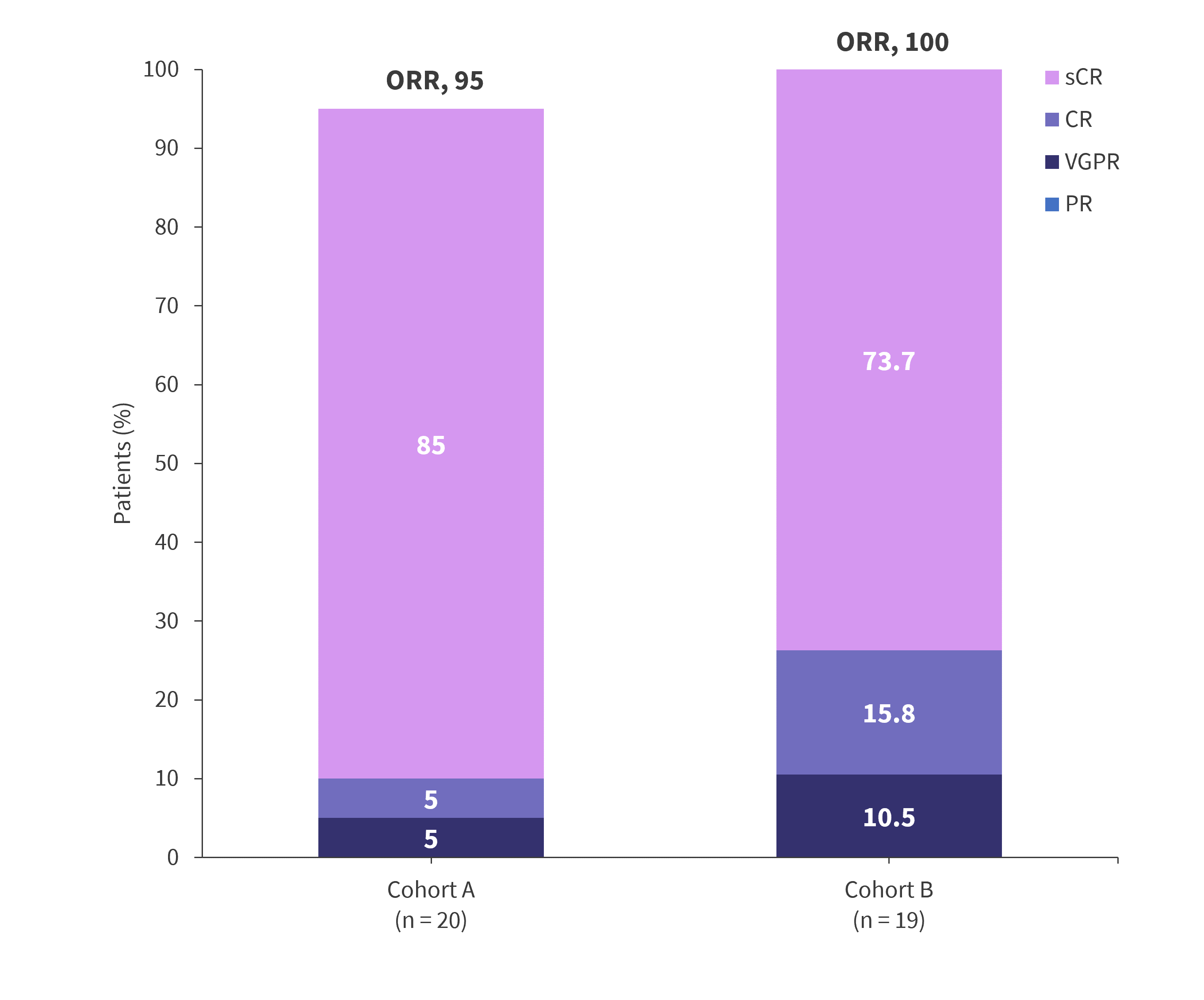
CR, complete response; ORR, overall response rate; PR, partial response; sCR, stringent complete response; VGPR, very good partial response.
*Data from Hillengrass, et al.4
At 24 months, median overall survival, PFS, and duration of response were not reached in either cohort (Figure 5).
Figure 5. 24-month OS, PFS, and DOR from CARTITUDE-2*
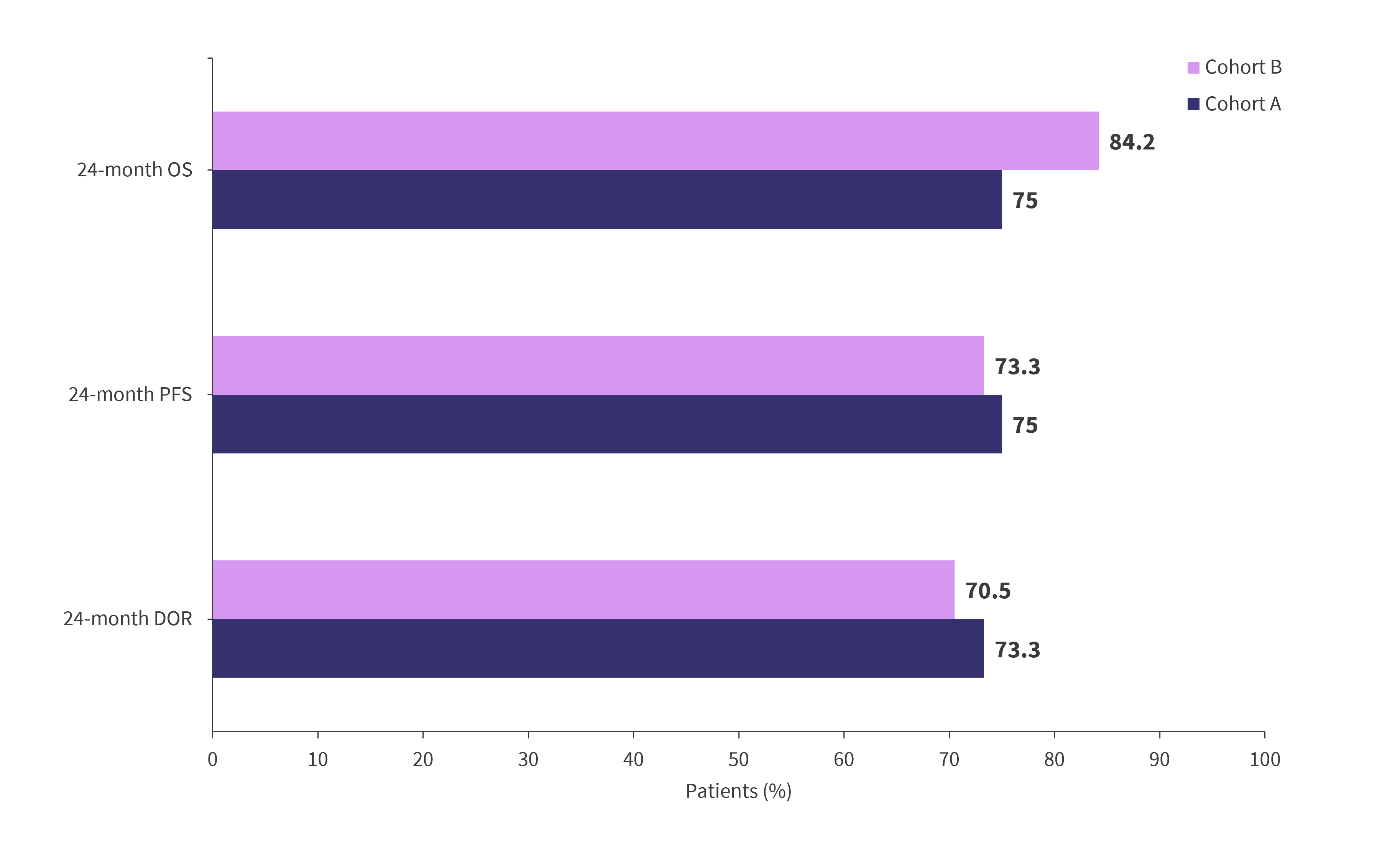
DOR, duration of response; OS, overall survival; PFS, progression-free survival.
*Data from Hillengrass, et al.4
Safety3
- Rates of adverse events, and particularly CRS, remained high: 95% and 84.2% in cohorts A and B, respectively. However, rates of Grade 3 or 4 events were markedly lower, at 10% and 5.3% (Table 1).
- Treatment-emergent cytopenias, such as neutropenia, lymphopenia, and thrombocytopenia, were common in both cohorts, with a high proportion of Grade 3/4 events, consistent with cilta-cel use in later lines.
- Secondary primary malignancies (SPMs) are being investigated increasingly for their association with CAR T-cell therapies, with SPMs only observed in cohort B.
- However, due to a small cohort size, these proportions are likely unrepresentative of the larger population.
Table 1. Cytopenias and adverse events of special interest from CARTITUDE-2*
|
Adverse events, % |
Cohort A |
Cohort B |
||
|---|---|---|---|---|
|
Any grade |
Grade 3/4 |
Any grade |
Grade 3/4 |
|
|
Treatment-emergent cytopenias |
|
|
|
|
|
Neutropenia |
95 |
95 |
94.7 |
89.5 |
|
Lymphopenia |
80 |
80 |
47.4 |
47.4 |
|
Thrombocytopenia |
80 |
40 |
57.9 |
26.3 |
|
Anemia |
75 |
45 |
57.9 |
47.4 |
|
Leukopenia |
60 |
60 |
31.6 |
31.6 |
|
AEs of special interest |
|
|
|
|
|
CRS |
95 |
10 |
84.2 |
5.3 |
|
CAR T-cell neurotoxicity |
30 |
5 |
31.6 |
5.3 |
|
ICANS |
15 |
0 |
5.3 |
0 |
|
Other neurotoxicities |
15 |
5 |
26.3 |
5.3 |
|
MNT |
0 |
0 |
5.3 |
5.3 |
|
SPM |
0 |
0 |
10.5 |
5.3 |
|
AE, adverse event; CAR, chimeric antigen receptor; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; MNT, movement/neurocognitive treatment-emergent adverse event. |
||||
CARTITUDE-4
CARTITUDE-4 (NCT04181827) is a phase III, randomized trial evaluating the safety and efficacy of cilta-cel in patients with lenalidomide-refractory MM after one to three prior lines of therapy. The control group was standard-of-care treatment consisting of pomalidomide, bortezomib, and dexamethasone or daratumumab, pomalidomide, and dexamethasone.
The trial design of CARTITUDE-4, including primary and secondary endpoints, has been reported previously by the Multiple Myeloma Hub here.
Efficacy
High rates of overall response were observed in the 176 patients enrolled in CARTITUDE-4, with a majority (86.4%) reaching a complete response or higher (Figure 6).
Figure 6. Response rates from CARTITUDE-4*
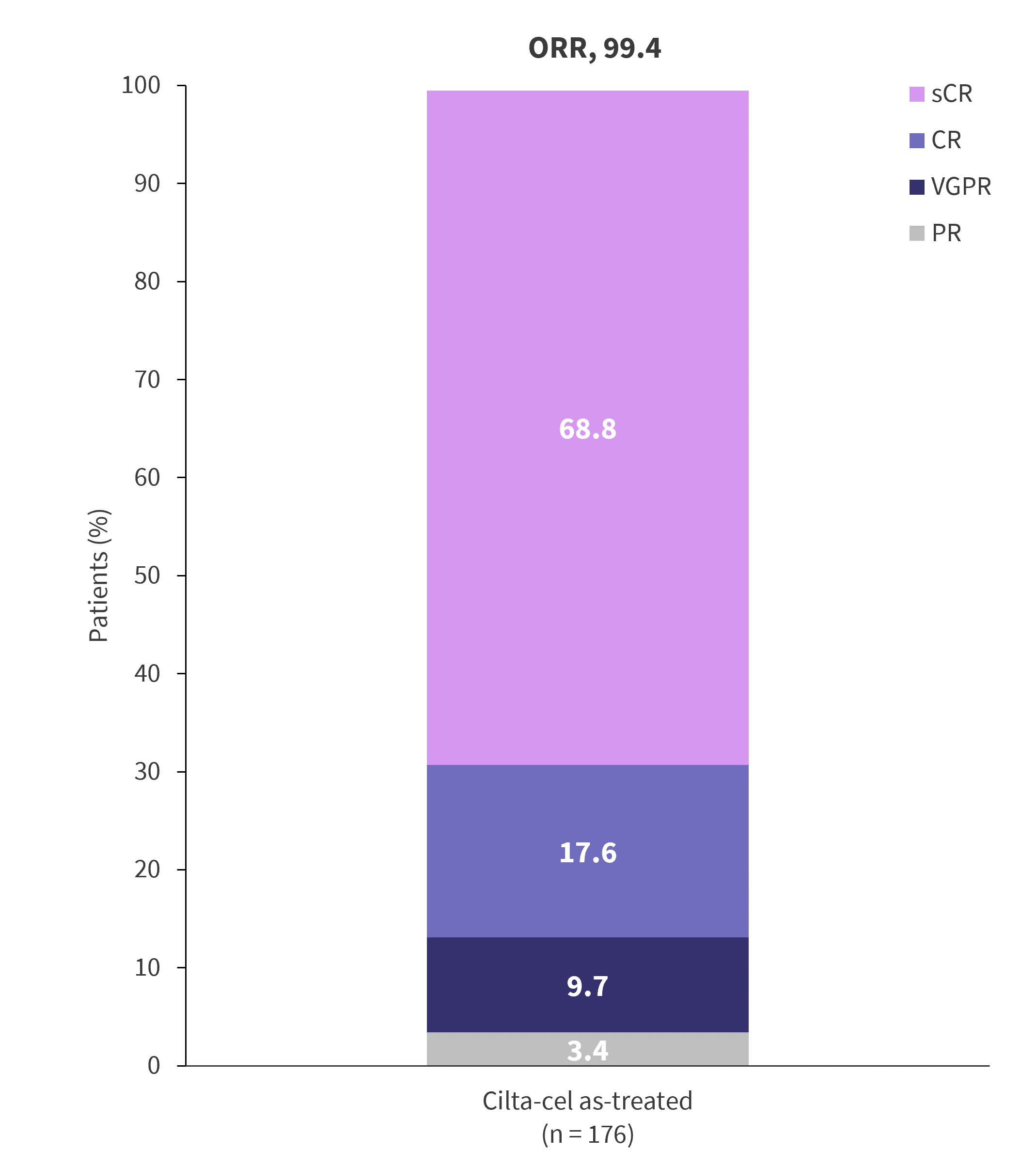
CR, complete response; ORR, overall response rate; PR, partial response; sCR, stringent complete response; VGPR, very good partial response.
*Adapted from Einsele.2
Safety2
As compared with CARTITUDE-1, a trial of cilta-cel in RRMM four or more prior lines of therapy, a lower incidence and severity of CRS, ICANS, and MNTs was observed in CARTITUDE-4, highlighting the potentially increased tolerability of CAR T-cell therapies in earlier lines. However, these data are likely confounded by differences in patient populations and treatment regimens, requiring further direct clinical trial comparisons to draw any conclusion.
Common adverse events included CRS and neurotoxicity, consistent with CAR T-cell use in later lines. However, the majority of these adverse events were Grade 1 or 2, with most cases of CRS resolved after 3 days (Table 2).
Table 2. Adverse events from CARTITUDE-4*
|
Adverse event, % unless otherwise specified |
As-treated patients (n = 176) |
||||
|---|---|---|---|---|---|
|
Any grade |
Grade 3/4 |
Median time to onset, days |
Median duration, days |
Resolved, n |
|
|
CRS |
76.1 |
1.1 |
8 |
3 |
134 |
|
Neurotoxicity |
20.5 |
2.8 |
- |
- |
- |
|
ICANS |
4.5 |
0 |
10 |
2 |
8 |
|
Other |
17 |
2.3 |
- |
- |
- |
|
Cranial nerve palsy |
9.1 |
1.1 |
21 |
77 |
14 |
|
Peripheral neuropathy |
2.8 |
0.6 |
63 |
201 |
3 |
|
MNT |
0.6 |
0 |
85 |
- |
0 |
|
CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; MNT, movement/neurocognitive treatment-emergent adverse event. |
|||||
CAR T-cell therapy in the first line1
Multiple trials investigating the safety and efficacy of CAR T-cell therapies in the first line setting in newly diagnosed MM are ongoing; including:
- CARTITUDE-5 (NCT04923893)
- Phase 3 randomized trial of bortezomib-lenalidomide-dexamethasone, followed by cilta-cel or followed by lenalidomide-dexamethasone in newly diagnosed MM where transplant is not planned as initial therapy
- Status: Ongoing
- CARTITUDE-6 (NCT05257083)
- Phase 3 randomized trial of daratumumab-bortezomib-lenalidomide-dexamethasone followed by cilta-cel or autologous stem cell transplant in newly diagnosed MM
- Status: Recruiting
Conclusion
A multitude of data support the investigation of cilta-cel in earlier lines of therapy, particularly highlighting the reduced likelihood of prior exposure to BCMA-directed therapies and lower incidence of toxicities, which have the potential to improve quality of life. Increased attrition rates paired with this reduction in toxicities highlight where CAR T-cell therapy may become appropriate and tolerable to a higher proportion of patients with MM. Data from CARTITUDE-2 and CARTITUDE-4 provide evidence for the efficacy of cilta-cel in this setting, although in relatively small cohorts.
This educational resource is independently supported by Johnson & Johnson. All content is developed by SES in collaboration with an expert steering committee; funders are allowed no influence on the content of this resource.
30 votes - 2 days left
- Janssen Receives Positive CHMP Opinion for CARVYKTI®▼ (ciltacabtagene autoleucel; cilta-cel) for Treatment in Earlier Lines of Relapsed and Refractory Multiple Myeloma. https://www.jnj.com/media-center/press-releases/janssen-receives-positive-chmp-opinion-for-carvykti-ciltacabtagene-autoleucel-cilta-cel-for-treatment-in-earlier-lines-of-relapsed-and-refractory-multiple-myeloma#:~:text=About%20Ciltacabtagene%20Autoleucel%20(cilta%2Dcel)&text=In%20February%202022%2C%20the%20U.S.,an%20anti%2DCD38%20monoclonal%20antibody. Published February 23, 2024. Accessed Mar 8, 2024.
- Einsele H. Moving CAR-T into first-line therapy in Multiple Myeloma. Physician session #PS08-1. Presented at: 6th European CAR T-cell Meeting; Feb 17, 2024; Valencia, ES.
- D’Agostino M and Raje N. Anti-BCMA CAR T-cell therapy in multiple myeloma: Can we do better? Leukemia. 2020;34(1):21-34. DOI: 1038/s41375-019-0669-4
- Hillengass J. The phase 2 Cartitude-2 trial: Updated efficacy and safety of ciltacabtagene autoleucel in patients with multiple myeloma and 1–3 prior lines of therapy (cohort A) and with early relapse after first line treatment (cohort B). Oral abstract #42. Presented at: 2024 Transplantation and Cellular Therapy Meetings of the ASTCT and CIMBTR; Feb 23, 2024; San Antonio, US.
Your opinion matters
30 votes - 2 days left ...
Newsletter
Subscribe to get the best content related to multiple myeloma delivered to your inbox